Well folks, I sure didn’t expect my first article on this new website to talk about a global pandemic. I would have expected an exposé on 5G or a heavy-hitting commentary on Elon Musk’s current crazy plan to send up to 42,000 EMF-beaming satellites in space. But here we are.
I must say that, like it happened for a lot of people, the COVID-19 (coronavirus) crisis caught me completely off guard at first, and left me with a perfectly dangerous mix of anxiety and depression. “I’m done reading about the coronavirus,” I told my wife and business partner Gen a few days ago. “This is not my battle.”
But that very afternoon, I received an email from one of my international collaborators — one who frequently sends me updates on the development of wireless technologies — that would completely change my mind.
“Nick…” he said (quoting him loosely), “A lot of people want to know your calm perspective on this whole situation. I think the best thing you can do to calm down your anxiety levels is not to ignore the issue, but the exact opposite… do more research, and simply publish what you’ve found so far.” It hit home big time, and I got to work.
My goal with this article is not to claim I have all the answers, because I definitely don’t. This is my attempt at bringing a balanced perspective on a global issue which affects every one of us, and one that is clouded by a massive amount of fear.
| Note: Please note that the information below has been last updated on April 1st, 2020, so by the time this gets published, it’s possible that certain parts will have already become irrelevant or inaccurate. This is the nature of such a fast-paced, media-frenzied crisis.
This article reflects my current understanding of the situation. That understanding has its limitations, one being that viral epidemiology and statistics are relatively new topics for me compared to EMF science and other areas I’ve spent years studying. If you see glaring mistakes in the article, please contribute to a healthy discussion below (and help me and others in the process) and don’t let that deter you from the main point: The clear disconnect between the available scientific data and our reaction to COVID-19. If inaccuracies are found or new information comes to light, I might update this article, in which case I’ll include a description of the changes I’ve made in this box.
|
Table of Contents
Fact #2: “Confirmed” Cases Of COVID-19 Are… Well… Not-So-Confirmed
Fact #3: “Confirmed” Deaths From COVID-19 Are Not-So-Confirmed Either
Fact #4: The WHO’s Panic-Inducing Death Rates Are Akin To Comparing Apples To Oranges
Fact #5: Overall Mortality Rates From Respiratory Infections Have Still Not Increased Significantly
Fact #7: The Data Confirms That Lockdowns Are Possibly Useless & Surely Damaging
Fact #8: Things Are Getting Better, And Better, And Better
The Anti-Conclusion: What This Article Does Not Claim
Conclusion: What This All Means & What You Should Do
Warning: I’m a Contrarian.
Let’s get this out of the way right off the bat.
I’m a contrarian. It’s how my brain operates. This means I have a propensity to be fascinated by people who have views opposite from everyone else.
This trait can definitely be considered a strength in certain scenarios. For instance, it helped me become so obsessed with the idea that we might have been told a big, blatant lie about how wireless radiation is “perfectly safe” — that I spent thousands of hours researching the topic, and ended up writing an entire book about it. Now I have no doubt wireless radiation is unsafe, which is 50% comforting, and 50% depressing.
When I first heard about this entire COVID-19 situation, I was late in the game; and got caught completely off guard by how huge (that’s an understatement) the whole thing had rapidly become.
I don’t watch TV, and greatly limit how much information I consume from mainstream media — especially when it comes to EMFs. After all, it’s clear that the vast majority of mainstream news outlets very rarely debate cell phone safety or report on how reckless our use of wireless radiation currently is. Quite probably because their editorial guidelines are influenced by advertising money coming from tech giants and Telecoms.
(On the contrary, independent media outlets in the US like The Nation, The New Yorker, The Epoch Times, and many others have often reported on various issues related to wireless radiation and 5G.)
I started diving into the coronavirus story and rapidly found people on both sides of that story. Certain people were claiming that millions of people would die if we don’t act fast, while contrarians were (of course!) claiming that this entire story was a “hoax”.
I watched “preppers” claiming this was “it”, and that the society was collapsing and that we should have prepared better. I heard health officials claiming that millions of lives were at stake. I heard scientists say that on the contrary, the entire situation was completely overblown. I saw people fearing for their life. And I’m guessing that like it might have happened for you, I quickly didn’t know who to believe.
“Well…” I thought, “On the one hand I hope that those who claim COVID-19 is not as dangerous as everyone claim it is are right, since that would mean we’re actually not facing a major health threat and we can all calm down. But on the other hand I sure hope they are wrong — or we may have made a terrible mistake in the way we reacted.”
After spending day and night studying the issue in the last weeks, I identified 8 very inconvenient facts that are mostly missing from current discussions and reporting on COVID-19. Without further ado, here’s my honest attempt at looking at the situation calmly and rationally.
Fact #1: We’re Locking Down Entire Countries To Stop the Coronavirus… And The Consequences Are (And Will Be) Disastrous
Let’s start with the very obvious: Our war against this new virus has been extremely costly, and it’s only the tip of the iceberg.
I’m not an expert in finance, but it doesn’t take one to see that the COVID-19 crisis has inflicted major damage to the world’s economy. S&P Global reports that “COVID-19 could knock US$211 billion [emphasis mine] from Asia-Pacific incomes and slow GDP growth to 4.0% in 2020.”
Some industries are already considering the “coronavirus shock” the worst financial meltdown in history, worse than both the 2008-2009 global financial crisis and the Wall Street Crash of 1929.
I’m sitting here at my desk in Quebec’s beautiful countryside, on day 8 of a 14-day self-quarantine that has been heavily recommended at first, then quickly mandated (the fine is up to $750K) by public health officials to Canadians returning from abroad.
Everything is closed down except grocery stores and convenience stores (“dépanneurs” as we call them in Quebec). Oh but the SAQ (alcohol stores) and SQDC (cannabis stores) are staying open after all. After all, people need something to pass the time.
The entire society is frozen. This lockdown situation will last for at least 3 more weeks, but schools and shopping malls will stay closed until at least May 1st.
The economical downside of paralyzing the entire province for a few weeks is quite obvious. Small and large businesses have already started laying off thousands of people, and those with the lowest incomes are extremely likely to not have any paid leave and therefore suffer the most from that situation. (Quebec and Canada alike have announced financial support measures for those affected).
Like many other governments around the world, the Canadian government is discussing the possibility of using the “War Measures Act” (now called “Emergencies Act” to tone down the fear a bit) should the situation become even worse.
France is on lockdown, with 100,000 policemen patrolling the streets. Several other countries in the EU are either on lockdown or plan to do the same. India just announced a 21-day lockdown. The US has extended their social distancing measures to April 30th. You get the idea — these extreme pandemic-containment measures are being implemented practically everywhere, and they are devastating.
We’re being told that these extreme measures are necessary to save lives, a lot of them. According to the Center for Disease Control (CDC), deaths from Covid-19 could range from 200,000 to 1.7 million people in the U.S. alone.
Dedicated to the incredible human beings fighting to put safety before profits.
The dedication you can find at the beginning of my 2017 book, The Non-Tinfoil Guide to EMFs.
I didn’t dedicate my book to those who “put safety before profits” for nothing. If we can save all of these people, prevent all of these deaths, then the economical sacrifice might be worth it in the end.
I just hope with all my heart these guys got their numbers right.
| Bottom line: Extreme interventions to stop the COVID-19 pandemic have been devastating to the economy, but are claimed to be able to save millions of lives. |
Fact #2: “Confirmed” Cases Of COVID-19 Are… Well… Not-So-Confirmed
This is where we’ll start getting geeky a bit, but it’s for a good cause:
If we are to take such extreme measures to stop a virus and do unprecedented economical damage in the process, we absolutely need to ensure that all the decisions being taken by world leaders are based on solid, unbiased scientific data.
Unfortunately, the more I dive into the topic, the more shaky the science behind our assessment of the current situation is looking — beginning with how we confirm that people are infected with COVID-19. This situation sure reminds me of the shock I felt when I first discovered that cell phone safety tests are completely bogus (one example here) several years ago.
There are several glaring problems with the RT-PCR test that’s used to detect the presence of the SARS-CoV-2 virus which is said to cause the new COVID-19 disease (the WHO explains the difference between these two terms here). I’ll deconstruct what I consider to be the most important ones below, but if you want to go deeper down that rabbit hole, then review David Crowe’s lengthy and detailed critique on the topic.
Testing Problem #1: The RT-PCR test does not rule out bacterial infection or co-infections with other viruses.
Hey, I’m not making this up — it’s clearly stated in the CDC COVID-19 testing kit’s instruction manual.
- “Positive results are indicative of active infection with 2019-nCoV but do not rule out bacterial infection or co-infection with other viruses. [emphasis mine]
- The agent detected may not be the definite cause of disease (we’ll come back to this one soon)
In other words, the test can detect the presence of the RNA of the virus SARS-CoV-2, but does not rule out the fact that a person considered a “confirmed” case of COVID-19 might also have a serious (or deadly) bacterial infection, or even other viruses which might be responsible for their symptoms.
But in the current political and medical climate, the vast majority of those who test positive will be considered a “confirmed” case of COVID-19, regardless of whether their actual symptoms are caused by COVID-19, or by something else.
We can also rest assured that should this symptomatic person die, the cause of death will be likely be “COVID-19”, and not “they had COVID-19 but also several viruses and bacteria co-infections that each might have contributed to their death”. And they will become another red dot on the Johns Hopkins Coronavirus Tracker.
Sidenote: In a quiet PR move, the CDC removed an important word from their documentation somewhere between March 14th and March 16th, probably because they didn’t want to have people question how reliable the tests are. Instead of saying that the test will lead to the “presumptive identification” of COVID-19 (which it does), it now says that the test will lead to the “identification” of COVID-19.
|
|

March 16th, 2020 version. Thanks to Anette Iren Isene from the Facebook group Balance Nation for this discovery. |

Testing Problem #2: Up to 80% false positives?
Okay, this is one study. But if that number happens to be true, then we are in deep, deep trouble — since this might mean our entire assessment of the current situation might be wrong by orders of magnitude.
In their study titled, “[Potential False-Positive Rate Among the ‘Asymptomatic Infected Individuals’ in Close Contacts of COVID-19 Patients]”, Chinese researchers Zhuang et al. reported on March 5th 2020 that:
“When the infection rate of the close contacts and the sensitivity and specificity of reported results were taken as the point estimates, the positive predictive value of the active screening was only 19.67%, in contrast, the false-positive rate of positive results was 80.33%. [emphasis mine]”

A false-positive is when a test shows that someone has been infected with the coronavirus, when in reality they have not been infected.
But this gets more complicated, since false-negatives might also be a serious problem. In other words, people are being told they don’t have the virus when in reality they have it. Both of these problems with testing makes our assessment of how big the issue is much more blurry.
IMPORTANT March 26th update: Since I first wrote this part, it was confirmed that the original Chinese study has been retracted, as confirmed by NPR. We currently do not know a lot about why it was retracted, other than the senior author of that study saying it’s because of a “sensitive matter”. The rest is up to speculation.
Even if this study ends up being proven false, there are several other indications that the tests might be inaccurate, something that in the end needs to be part of the scientific and public debate:
- Wang Chen, president of the Chinese Academy of Medical Sciences admitted in early February that “the accuracy rate of the test is only 30 to 50 percent.”
- 14% of ‘recovered’ patients in China test positive again for SARS-CoV-2. This is downright bizarre and supports the idea that they were in fact never infected with the virus (false-positives).
- The rapid tests measuring antibodies which have been considered a possible alternative to test large samples of population are also extremely inaccurate. The Spanish media El Pais report that “the tests acquired by the Government have a sensitivity of 30% when they should exceed 80%”.
Testing Problem #3: The WHO & world governments have complete faith in these clearly inaccurate tests
Even though the tests are clearly not reliable, the WHO and governments around the world seem to be taking their results at face value, a fact that David Crowe describes in length in his article:
“Infectious diseases always have a definition, but they are usually not publicized too widely because then they would be open to ridicule. They usually have a ‘suspect case’ category based on symptoms and exposure, and a ‘confirmed’ category that adds some kind of testing”.
Since January 18th, after Chinese researchers gathered more information on this novel virus, the definition of a suspect case of COVID-19 changed to these 4 criteria:
- Fever, with or without recorded temperature (Crowe notes that this criterion is as vague as it can get.)
- Radiographic evidence of pneumonia
- “Low or normal white-cell count or low lymphocyte count” (Crowe notes: “This is not really a criterion as every healthy person is included.”)
- One of these two:
- Patient has a travel history to Wuhan, OR
- Direct contact with patients from Wuhan who had a fever or respiratory symptoms, within 14 days before illness onset
Confirmed cases of COVID-19 were defined by the WHO as “a person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms.” [emphasis mine]
Crowe continues:
The big problem is that, in contrast to the definition for SARS, a ‘confirmed case’ did not originally require the criteria for a suspect case to be met. A ‘confirmed case’ simply required a positive RNA test, without any symptoms or possibility of contact with previous cases, illustrating total faith in the PCR technology used in the test. The World Health Organization definition has the same flaw.
It was the fact that the SARS definition required both a reasonable possibility of contact with a previous case, and symptoms, that allowed the epidemic to burn out. Once everyone was quarantined, new cases were highly unlikely, testing stopped, and doctors could declare victory.
In plain English: Anyone who tests “positive” on the RT-PCR test, which is known to be extremely inaccurate, can be considered a “confirmed case” of COVID-19, even if there’s no way on Earth that person could have ever been in contact with someone infected with COVID-19.
But this part gets even more interesting, and might explain why COVID-19 “cases” in China decreased so much around mid-February.
The Chinese eventually woke up and, around February 16th required confirmed cases to meet the requirements for a suspected case, as well as a positive test.
They may have put this new definition into practice earlier because after a massive addition of almost 16,000 confirmed cases on February 12th, the number fell dramatically each day and, by February 18th was under 500 cases, and continued to stay low. [emphasis mine]
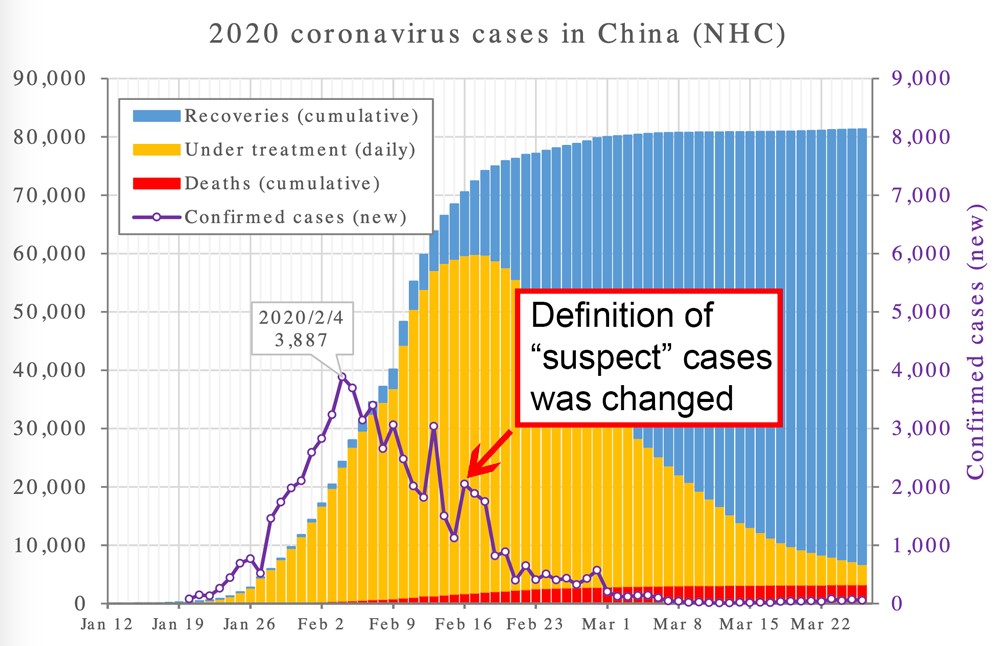
Image credit: Adapted from a photo by Phoenix7777. I added arrows and text to highlight the fact that the number of cases has dropped since February 16th. https://upload.wikimedia.org/wikipedia/commons/e/e5/2020_coronavirus_patients_in_China.svg / CC BY-SA 4.0
But other countries did not learn. Korea, Japan and Italy (and perhaps other countries) have started doing tests on people with no epidemiological link, encouraging people with the vague symptoms that are part of the definition to come to the hospital to get checked out, and obviously following up with asymptomatic people with a connection to anybody who tests positive. Consequently, in mid to late February, cases in those countries started to skyrocket.
This part is so important it bears repeating. With such an imprecise test, there’s a strong chance that the more you test, the more so-called “confirmed cases” of COVID-19 you get. The more you will see “outbreaks”. The more panic you create. And the less scientific and rational your assessment of the whole situation becomes.
As I was right about to publish this article, new data came to light that reinforced the idea that this pandemic is at least partially a pandemic of testing:
Recent data from the German Robert Koch Institute show “that the increase in test-positive persons is proportional to the increase in the number of tests (i.e. in percentage terms it remains roughly the same). This may indicate that the increase in the number of cases is mainly due to an increase in the number of tests, and not due to an ongoing epidemic” (As reported by Swiss Propaganda Research (“SPG”)).
At the same time, “German researcher Dr. Richard Capek argues in a quantitative analysis that the ‘Corona epidemic’ is in fact an ‘epidemic of tests’. Capek shows that while the number of tests has increased exponentially, the proportion of infections has remained stable and mortality has decreased, which speaks against an exponential spread of the virus itself. (idem — SPG)

Testing Problem #4: More inconsistencies
On February 27th 2020, a group of doctors from Marseilles, France published very surprising findings. After testing more than 4,000 respiratory samples using “several systems, including those released at the European level”, they found a grand number of… zero SARS-CoV-2 cases.
The respiratory samples they used included samples from 32 suspected cases of COVID-19, 337 people who had just returned from China who were tested twice, and 164 French patients who died from respiratory illnesses from 2014 to 2019 (to verify if the virus had been around for longer than previously thought).
The research group concluded:
It is surprising to see that all the attention focused on a virus whose mortality ultimately appears to be of the same order of magnitude as that of common coronaviruses or other respiratory viruses such as influenza or respiratory syncytial virus [emphasis mine], while the four common HCoV [other coronaviruses] diagnosed go unnoticed although their incidence is high.
The same research group was very critical of the MERS epidemic of 2012, after their lab had “highlighted the absence of diagnosis of this [MERS virus] among travellers returning from the Hajj pilgrimage, which contrasted with the considerable anxiety relating to this emerging infection and its risk of importation and spread in mainland France.”
They boldly added:
Seven years later, the emergence of SARS-CoV-2 in December 2019 reproduced this pattern of disproportionate fear of importation [emphasis mine] and spread of infections in mainland France while the cases reported worldwide remain almost only localised in China as only 34 people died of this disease (Covid-19) outside China as of February 25, 2020.
But that was an entire month ago, so one could argue the data is already “old”. Based on the data in France until March 3rd, that same group reported that “2.6 million deaths from respiratory infections (excluding tuberculosis) per year have been noted in recent years worldwide. There is little chance that the emergence of SARS-CoV-2 could change this statistic significantly. Fear could have a larger impact than the virus itself.”
(Note: At the time of this writing, death rates in France have gone up significantly. The same research group could come up with different conclusions based on the new numbers.)
Finally, as pointed out by the nonprofit organization Swiss Propaganda Research, American diagnostic manufacturer Creative Diagnostics specifies that “the detection result of this [COVID-19 test] is only for clinical reference, and it should not be used as the only evidence for clinical diagnosis and treatment [emphasis mine].” This directly goes against WHO’s definition of what is a “confirmed case”.
| Bottom line: The test used to confirm cases of COVID-19 is very inaccurate, which artificially inflates the total case count and makes it way harder to predict with accuracy how dangerous this potential threat really is. |
Fact #3: “Confirmed” Deaths From COVID-19 Are Not-So-Confirmed Either
You’ve guessed it — the story does get worse.
It turns out that just like a large fraction of “confirmed” cases of COVID-19 are possibly not real cases of COVID-19, a lot of deaths blamed on COVID-19 probably have nothing to do with COVID-19.
The tricky part is that so far, the vast majority of deaths attributed to COVID-19 have been seen in the older population, and that a lot of these folks have multiple other conditions that could have been responsible for their death.
There’s also the fact that since the COVID-19 test kits do not rule out the presence of a bacterial infection or of other viruses (such as the very common Influenza A or B), it’s quite possible that people who got killed by the seasonal flu or other viruses will in fact be counted as a victim of COVID-19.
This problem has been highlighted by Stanford Medicine Data scientists, who released their early findings which show that up to 25% of all people infected with SARS-CoV-2 also had a co-infection. They commented that “these co-infection rates are much higher than previously reported rates.”
And since we are in the midst of a global panic where everyone is looking for a new, deadly virus, it’s natural to think that the medical system will display a huge confirmation bias and artificially make COVID-19 appear more deadly than it really is.
Dr. John Lee, consultant histopathologist at Rotherham General Hospital, shares the same concerns:
In the current climate, anyone with a positive test for Covid-19 will certainly be known to clinical staff looking after them: if any of these patients die, staff will have to record the Covid-19 designation on the death certificate — contrary to usual practice for most infections of this kind. [emphasis mine] There is a big difference between Covid-19 causing death, and Covid-19 being found in someone who died of other causes. Making Covid-19 notifiable might give the appearance of it causing increasing numbers of deaths, whether this is true or not. It might appear far more of a killer than flu, simply because of the way deaths are recorded.
Here’s the problem: we know from recent Italian data (the example everyone uses in the media to prove how deadly this COVID-19 pandemic is) that 99% of all patients who presumably died from COVID-19 had other illnesses.
Investigative reporter Jon Rappoport reported on that story on March 17th:
There may be only two people who died from coronavirus in Italy, who did not present other pathologies. [emphasis mine] This is what emerges from the medical records examined so far by the Higher Institute of Health, according to what was reported by the President of the Institute [Istituto Superiore di Sanità (ISS), Italian National Institute of Health], Silvio Brusaferro, during the press conference held today at the Civil Protection in Rome.
…At present, in fact, the authorities are unable to distinguish those who died from the virus from those who, on the other hand, are communicated daily to the public, but who were mostly carriers of other serious diseases and who, therefore, would not have died from Covid-19. In response to a question from ‘Agenzia Nova’, in fact, Brusaferro was unable to indicate the exact number of coronavirus deaths. However, the professor clarified that, according to the data analyzed, the vast majority of the victims ‘had serious [non-COV] pathologies’ and in some cases the onset of an infection of the respiratory tract can lead more easily to death.
As reported by SPG, Italian Professor Walter Ricciardi agrees with this analysis and admits that:
Only 12% of death certificates have shown a direct causality from coronavirus, whereas in public reports all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus. ‘This means that Italian death figures reported by the media have to be reduced by at least a factor of 8 to obtain actual deaths caused by the virus. [emphasis mine] Thus one ends up with at most a few dozen deaths per day, compared to an overall daily mortality of 1800 deaths and up to 20,000 flu deaths per year’.
Considering that a whopping 68,000 Italians have died from the flu during 4 recent flu seasons, this begs the serious question whether COVID-19 is the sole culprit of what has been reported as a medical apocalypse in the media.
More recently, the major outbreak in New York City has started to steal the attention — causing 1,550 “confirmed deaths” as of March 31st.
But again, the same problem can be seen, as highlighted by physician Dr. Anthony G. Beck in a recent video. In the latest NYC Health’s Coronavirus Disease 2019 (COVID-19) Daily Data Summary, 80.3% of all people who died while having tested positive for COVID-19 had “underlying illnesses including diabetes, lung disease, cancer, immunodeficiency, heart disease, hypertension, asthma, kidney disease, or GI/liver disease”.
Is Smog Clouding Our Analysis?
A lot of what is currently blamed across the board on COVID-19 could be a mixed bag of COVID-19 deaths, deaths from influenza (including the possibility of a very deadly flu season) or other viruses, pneumonias from many other causes (including antibiotic-resistant bacteria, which kill 10,000 Italians yearly) and the consequences of living in one of the most polluted air in all of Europe, day in and day out.
Already in November of 2019, before the whole COVID-19 situation broke out, a leading Italian physician was reporting what he called “strange cases of pneumonia” in the Lombardy region. The region around Italy’s capital, Milan (the most affected so far by COVID-19) has the 2nd worst smog in all of Europe, an environmental factor which both diminishes people’s ability to fight viruses and helps propagate viruses faster.
Italians are also known to willingly pay to breathe smog — I’m taking about smoking, of course — and this kills about 80,000 of them every year.
And as if it were not bad enough, a 2003 Chinese study concluded that you’re 84% more likely to die from SARS if you’re exposed to moderate air pollution compared to people who breathe clean air. If you live in a heavily polluted area, this risk goes up by 200%. This could very well also be true for other viruses.
What is even more damning is that doctors worldwide are simply unable to accurately recognize cases of COVID-19 based on clinical symptoms alone. That’s why the White House Coronavirus Response Coordinator, Dr. Deborah Birx, reminded everyone on March 14th that: “South Korea saw a 96% or more negative testing rate even though they were testing people with symptoms.” [emphasis mine]
This clinical inability to recognize COVID-19 adds confusion to the confusion, and makes it extremely likely that a lot of “confirmed cases” and “confirmed deaths” of COVID-19 are in fact something else entirely.
| Bottom line: Just like “confirmed” cases of COVID-19 could easily be false-positives, a large fraction of “confirmed” deaths from COVID-19 could be due to something else. The WHO recognizes that up to 1,780 people die from the flu every single day worldwide, while in 2016 about 2,961 adults 70 years and older died every single day just from lower respiratory infections. |
Fact #4: The WHO’s Panic-Inducing Death Rates Are Akin To Comparing Apples To Oranges
On March 3rd, Tedros Adhanom — Director general of the World Health Organization — made a statement that made a lot of people panic.
“Globally” he said, “about 3.4 percent of reported COVID-19 cases have died. By comparison, seasonal flu generally kills far fewer than one per cent of those infected.”
The math used by Adhanom was surprisingly out of context, and in my opinion downright irresponsible given the media hysteria that ensued.
Yes, COVID-19 did show a fatality rate of 3.4% when the announcement was made. That’s 3,110 deaths out of 90,893 “confirmed” cases (keeping in mind that a lot of these confirmed cases and confirmed deaths are probably not related to COVID-19 at all).
But comparing these early numbers to the 0.1% death rate of the seasonal flu is simply ludicrous — since the flu’s death rate is calculated not by dividing deaths by the amount of flu cases that have been confirmed via testing, but by dividing deaths by the estimated amount of people who got the flu during that season. The chart below will make things clearer:
| 2019-2020 | Seasonal Flu – US | COVID-19 – US | COVID-19 – Global |
| Number of Deaths | 23,000 | 737 | 21,181 (March 25th) |
| Confirmed Cases (through testing) | 231,654 | 54,453 | 467,594 |
| Estimated Cases (mathematical models) | 38,000,000 | Unknown | Unknown |
| Death Rate / Confirmed Cases | 9.9% | 1.3% | 4.5% |
| Death Rate / Estimated Cases | 0.06% | Unknown | Unknown |
Adapted from a chart found at TheGatewayPundit.com. COVID-19 Numbers taken from the Johns Hopkins COVID-19 Tracker and the CDC’s website on March 25th, 2020. 2019-2020 flu season numbers are from the CDC’s Weekly U.S. Influenza Surveillance Report.
There’s a huge difference between 9.9% and 0.06%, right? That’s the difference between a regular flu season which doesn’t even get media attention and the next Spanish flu epidemic which wipes millions of people off the face of the planet.
If we really wanted to compare apples to apples, COVID-19 was half as deadly as the seasonal flu when Adhanom made his announcement, and not 30+ times deadlier like some have tried to argue.
Of course, we’re not comparing the right apples here, since comparing the deaths / total estimated cases ratio would be the fairest comparison between the seasonal flu and COVID-19. There’s also the fact that there were early indications that COVID-19 had a very high R0 (basic reproduction number), a fact that contributed to the global concern.
That being said, the reality is that we cannot possibly determine what the final death rate from a pandemic will end up being while we’re still in the middle of it. The best we can do is use the data we have and estimate what the risk is — and act accordingly.
But there is such a thing as acting too soon, based on insufficient data, and out of fear, as John P.A. Ioannidis — professor of medicine and epidemiology at Stanford — pointed out on March 17th:
Reported case fatality rates, like the official 3.4% rate from the World Health Organization, cause horror — and are meaningless. […] Reasonable estimates for the case fatality ratio in the general U.S. population vary from 0.05% to 1%.
A population-wide case fatality rate of 0.05% is lower than seasonal influenza. If that is the true rate, locking down the world with potentially tremendous social and financial consequences may be totally irrational. [emphasis mine]
If we decide to jump off the cliff, we need some data to inform us about the rationale of such an action and the chances of landing somewhere safe.
Not all experts agree with Ioannidis on what the real mortality rate from COVID-19 will end up being, of course. Here are revised estimates that have been published in the last few weeks (keep in mind that this list is by no means complete, and that new data is coming out every single day):
- “Much less than 1%” (Fauci et al., February 28th)
- 0.04 to 0.12% (Japanese study, March 13th)
- 0.25 to 3% (Wilson et al., March 13th)
- 0.05 to 1% (Ioannidis, Stanford, USA, March 17th)
- 0.2% (Wu et al. March 19th identified a 1.4% symptomatic mortality rate, on which I’ve applied the fact that up to 86% of the entire population might be asymptomatic)
- 0.01% (Bendavid & Bhattacharya, Stanford, March 24th)
- 0.66% (Verity et al., March 30th)
More and more data comes out every day, and a large fraction of it points towards the fact the equally comforting (this is not as deadly as we thought it was) and scary (we might have screwed up the economy for nothing) conclusion that COVID-19 is not a fraction as dangerous as it’s been depicted to be during this worldwide panic.
| Bottom line: The meaningless early death rates that have been communicated to and by the WHO and the media caused a worldwide panic. In the meantime, many scientists argue that we need more quality data before we are able to accurately assess how dangerous this new threat really is, and what strategies might be appropriate to contain it. |
Fact #5: Overall Mortality Rates From Respiratory Infections Have Still Not Increased Significantly
If the COVID-19 “confirmed cases” and “confirmed deaths” based on inaccurate test kits cannot fully be trusted, if the real fatality rates are up to debate and if COVID-19 can easily be mistaken for something else… How on Earth can we assess how dangerous this virus really is?
SPG and several other scientists might have the answer:
“[…] The most important indicator for judging the danger of the disease is not the frequently reported number of positively-tested persons and deaths, but the number of persons actually and unexpectedly developing or dying from pneumonia (so-called excess mortality).” [emphasis mine]
Dr. Wolfgang Wodarg, a German pulmonologist, has been screaming the exact same thing from the internet rooftops for several weeks. In this stunning and sobering presentation, he explains:
I worked as a doctor and conducted a health department. I had my own sentinel, my own monitoring system for flu diseases. And every year I observed how many people became sick in an area of 150,000 inhabitants.Every new year — worldwide — we have new types of viruses because the viruses have to change themselves. […] There are about 100 different types of viruses that are changing constantly. Coronaviruses have always been part of them. [emphasis mine]
[…] What is missing at the moment is a rational way to look at things. We should ask questions like ‘How was it before?’, ‘Didn’t we have the same thing last year?’, ‘Is it even something new?’ That’s missing.
So, Dr. Wodarg, let’s ask the question: “Are more people dying from respiratory infections now than last year, when COVID-19 wasn’t around?”
Wodarg’s current assessment is that “There is no valid data and no evidence of exceptional health threats.” He continues, “The official mortality statistics, which are still available, and various national flu monitoring institutes show the normal course of the curves.”
Could this really be true? Let’s find out, and start with Italy — the most often cited example of how “deadly” this pandemic is:
Italy
The flu season is known to be particularly deadly in Europe, especially because of its aging population. During the 2013/14, 2014/15, 2015/16 and 2016/17 flu seasons, more than 68,000 italians died. It’s also known that hospitals in Northern Italy have been overwhelmed in recent flu seasons, and that Italians ICUs are known to run at 95-98% capacity (source: Prof. Ioannidis from Stanford) every Winter.
As of March 26th,
…the latest European monitoring report on overall mortality continues to show normal or below-average values in all countries and all age groups, but now with one exception: in the 65+ age group in Italy a currently increased overall mortality is predicted (so-called delay-adjusted z-score), which is, however, still below the values of the influenza waves of 2017 and 2018.
This goes against the common perception that “thousands of people have been killed by COVID-19 in Italy” and, for the moment, supports the idea that a lot of deaths attributed to COVID-19 are in fact due to a slew of other factors including the seasonal flu, respiratory illnesses and other pre-existing conditions.
Dr. Wodarg explains:
Even in Italy, without the new tests, the annual problem in the flu season would be observed [emphasis mine]: undersupply, an aging population, many deaths due to hospital infections, tightness, lack of staff and a high level of antibiotic resistance. A positive SARS-CoV-2 test is largely only a secondary finding. Influenza is still much more dangerous for weakened patients, but is hardly noticed.
Germany
The latest report (March 20th) from the Robert Koch Institute has confirmed that “the number of respiratory infections is now normalizing [like] in previous years without [any] lockdown.”

France
Just like Italy, France is an exception and has seen an increase in overall mortality in people 65 years and older.

At the moment, French authorities specify that “the share of the [COVID-19] epidemic in overall mortality remains to be determined.”
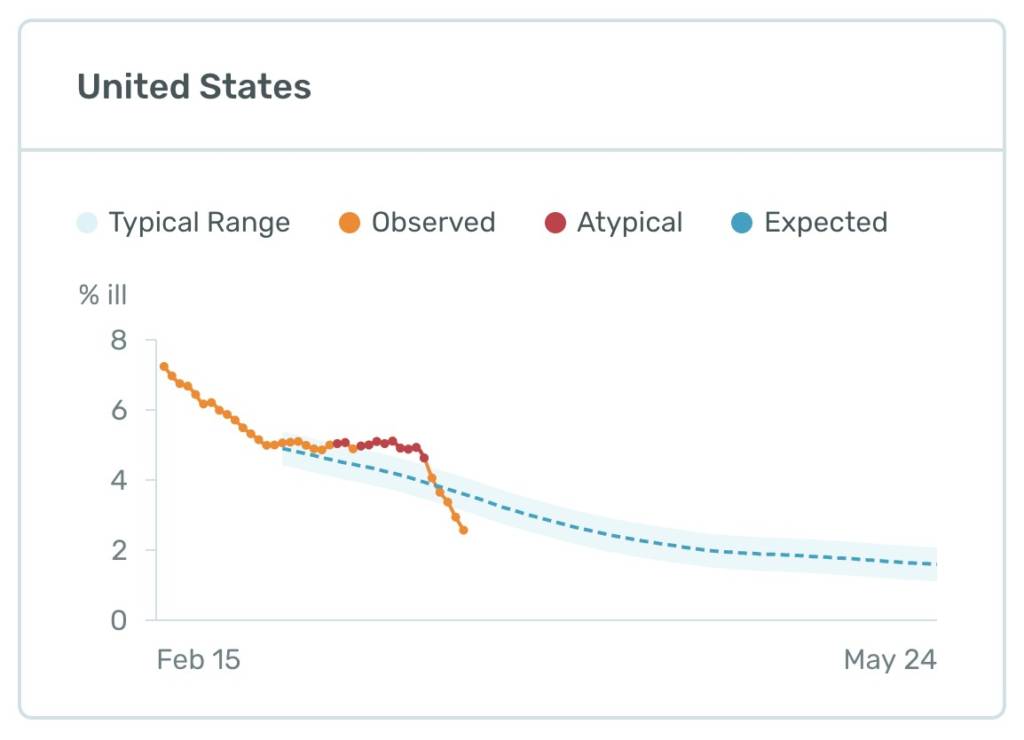
USA
The latest U.S. data coming out of the U.S. Health Weather Map as of March 25th show below- average levels of flu-like illnesses. Lockdown measures taken by the Trump administration can be ruled out since they have been in effect for just a few days.
Most people have no idea that up to 60,000 Americans die (2017-2018 season) from the flu every single year. So far, COVID-19 is claimed to have killed 4,476 (updated on April 1st), while the seasonal flu has killed at least 23,000 Americans in the last 5 months alone.
SPG also reports that:
Researcher Stephen McIntyre has evaluated the official data on deaths from pneumonia in the US. There are usually between 3000 and 5500 deaths per week and thus significantly more than the current figures for COVID-19. [emphasis mine] The total number of deaths in the US is between 50,000 and 60,000 per week. (Note: In the graph below, the latest figures for March 2020 have not yet been fully updated, so the curve is slumping).”

The Data Could Change, But Does Not Support The Most Dire Predictions
Now, it’s true that these numbers could change rapidly in the next few weeks and start showing a way different portrait. It’s also true that monitoring organizations such as the European monitoring of excess mortality for public action (MOMO) admit that “there is always a few weeks of delay in death registration and reporting. Hence, the EuroMOMO mortality figures for the most recent weeks must be interpreted with some caution.”
Still, the same stability in overall mortality can be seen in virtually all countries who have been touched by COVID-19 so far, which is a stark contrast to the “end of the world” panic sometimes displayed in the media.
To put things into perspective: For the moment, 45,497 total deaths (April 1st, Johns Hopkins Tracker) have been attributed to COVID-19. As a comparison, every single year around the world, an estimated 650,000 people die from flu-related respiratory death, an estimated whopping 1,080,958 adults older than 70 years die from lower respiratory infections and more than 2,600,000 people (source: Dr. Didier Raoult) die from all respiratory illnesses.
| Bottom line: More than 90 days into this COVID-19 situation, overall mortality rates from respiratory infections worldwide are still mostly normal, while being slightly elevated in France and Italy. This both supports the idea that many “confirmed deaths” attributed to COVID-19 might have been due to other factors, including influenza and other known causes of respiratory infections, while decreasing the odds that the doomsday predictions we’ve been hearing in the media will ever become a reality. |
Fact #6: A Slew Of International Experts Warn That The Danger Of COVID-19 Has Been Dangerously Overblown
The New York Times has developed a cool and useful tool on their website: two sliders where you can adjust the infection rate and fatality rate of COVID-19, and see how deadly it’s going to be.

In the intro of the article where they present their tool, they claim that “under a reasonable set of assumptions the number of fatalities could be high — potentially in the hundreds of thousands or more.”
This didn’t happen in China or any other country so far that has been touched by COVID-19, so these numbers are hypotheticals that in opinion are plain fear mongering and sensationalism at this point. And why on Earth would these sliders be able to go up to 7 million deaths, since the CDC’s most dire predictions (not supported by the data) are that 1.7 million Americans could die from this virus?
Around the world, scientists, doctors and a slew of experts are joining Dr. Wodarg in sharing the very unpopular and yet data-driven opinion that the fear mongering displayed by the media and the hysteria that followed need to stop. Since this means we might have destroyed the economy for no scientifically-valid reason, those who publicly speak out are unsurprisingly getting personally attacked by the media.
Here are some examples of world-class scientists who share the opinion that the COVID-19 situation is far from being as dangerous as it’s been depicted so far. [all emphasis below are mine]
“This is a pretty trivial pandemic. The word might seem shocking since people are dying, and considering the collective hallucinated drama we’re going through.
Still, the data is clear: respiratory infections kill approximately 2,600,000 people worldwide every single year. The same journalistic or political treatment we’ve seen for COVID-19 would cause just as much fear if we applied it to any regular flu season.”[my translation, source here]
– Didier Raoult, MD, PhD, rated #1 expert worldwide in Communicable Diseases, author of 2,300 indexed publications
“We are afraid that 1 million infections with the new virus will lead to 30 deaths per day over the next 100 days. But we do not realise that 20, 30, 40 or 100 patients positive for normal coronaviruses are already dying every day.
[The government’s anti-COVID-19 measures] are grotesque, absurd and very dangerous […] The life expectancy of millions is being shortened. The horrifying impact on the world economy threatens the existence of countless people. The consequences on medical care are profound. Already services to patients in need are reduced, operations cancelled, practices empty, hospital personnel dwindling. All this will impact profoundly on our whole society.
All these measures are leading to self-destruction and collective suicide based on nothing but a spook.”
– Dr. Sucharit Bhakdi, medical doctor and specialist in microbiology, one of the most cited research scientists in German history.
“Covid-19, has been called a once-in-a-century pandemic. But it may also be a once-in-a-century evidence fiasco. We are making decisions without reliable data.”
– John Ioannidis, professor of medicine, of epidemiology and population health, of biomedical data science, and of statistics at Stanford University and co-director of Stanford’s Meta-Research Innovation Center.
“Almost everyone I talk to, lay people and colleagues (I am a specialist in internal medicine and have worked for two years at a department of infectious diseases) consider the Coronavirus pandemic a pandemic of panic, more than anything else.
The panic looks like an unfortunate overreaction. We don’t even know if the risk of dying if you get infected with Coronavirus is higher than if you get influenza, or so many other virus infections, and most of those who die are old and suffer from comorbidity, just like for influenza.”
– Prof. Peter C. Gøtzsche, researcher and founder of the renowned Cochrane Medical Collaboration
“There is no valid data and no evidence of exceptional health threats. Without the tests, which are questionable in terms of their informative value and their falsifying application, there would be no indication for emergency measures.”
– Dr. Wolfgang Wodarg, Pulmonologist, Germany
“As an MIT PhD in Biological Engineering who studies & does research nearly every day on the Immune System, the #coronavirus fear mongering by the Deep State will go down in history as one of the biggest fraud to manipulate economies, suppress dissent, & push MANDATED Medicine!”
– Dr. Shiva Ayyadurai, MIT scientist who holds 4 PhD degrees and a researcher on the human immune system
*Dr. Shiva is very controversial to some, but I’ve chosen to include his quote since my goal is to present you with many different opinions in this article.
“Corona is not a serious killer virus! The scaremongering is the problem.”
– Prof. Dr. Karin Mölling, award-winning scientist and author of 250 papers
“The ill-founded opinions expressed by international experts, replicated by the media and social networks, repeat the unnecessary panic that we have previously experienced. The coronavirus identified in China in 2019 is no more dangerous than a strong cold or flu.”
– Dr. Pablo Goldschmidt, renowned virologist specialized in tropical diseases
“I have never seen anything like this, anything anywhere near like this. I’m not talking about the pandemic, because I’ve seen 30 of them, one every year. It is called influenza. And other respiratory illness viruses, we don’t always know what they are. But I’ve never seen this reaction, and I’m trying to understand why.
[…] I worry about the message to the public, about the fear of coming into contact with people, being in the same space as people, shaking their hands, having meetings with people. I worry about many, many consequences related to that.”
– Dr. Joel Kettner, professor of Community Health Sciences and Surgery at Manitoba University. His interview got cut off when he started expressing his honest opinion on the air.
“Italy is known for its enormous morbidity in respiratory problems, more than three times any other European country. […] In every country, more people die from regular flu compared with those who die from the coronavirus.
[..] There is a very good example that we all forget: the swine flu in 2009. That was a virus that reached the world from Mexico and until today there is no vaccination against it. But what? At that time there was no Facebook or there maybe was but it was still in its infancy. The coronavirus, in contrast, is a virus with public relations. Whoever thinks that governments end viruses is wrong.”
– Dr. Yoram Lass, Israeli physician, politician and former Director General of the Health Ministry
“I’ve been in this business for 30 years. […] I’ve been through MERS, SARS, Ebola, the first Gulf war and the second, and I don’t recall anything like this. There’s unnecessary, exaggerated panic. We have to calm people down.
[…] Everybody is whipping everybody else up into panic — the leaders, via the media, and the wider public — who then in turn start to stress out the leaders. We’ve entered some kind of vicious cycle.”
– Prof. Jihad Bishara, leading Israeli virologist and director of the Infectious Disease Unit at Petah Tikva’s Beilinson Hospital
“COVID-19 is no more dangerous than influenza (the flu), but it is simply observed much more closely. More dangerous than the virus is the fear and panic created by the media and the ‘authoritarian reaction’ of many governments.”
– Prof. Stefan Hockertz, Swiss infectious disease specialist
“In Italy, one in ten people diagnosed die, according to the findings of the Science publication, that is statistically one of every 1,000 people infected. Each individual case is tragic, but often – similar to the flu season – it affects people who are at the end of their lives.
[…] If we close the schools, we will prevent the children from quickly becoming immune. […] We should better integrate the scientific facts into the political decisions.”
– Dr. Pietro Vernazza, Swiss physician specializing Infectious Diseases at the Cantonal Hospital St. Gallen and Professor of Health Policy
“I am deeply concerned that the social, economic and public health consequences of this near total meltdown of normal life — schools and businesses closed, gatherings banned — will be long lasting and calamitous, possibly graver than the direct toll of the virus itself.
The stock market will bounce back in time, but many businesses never will. The unemployment, impoverishment and despair likely to result will be public health scourges of the first order.”
– Dr. David Katz, president of True Health Initiative and founding director of the Yale-Griffin Prevention Research Center
“I’m not a fan of lockdown. Anyone who imposes something like this must also say when and how to pick it up again. Since we have to assume that the virus will be with us for a long time, I wonder when we will return to normal?
You can’t keep schools and daycare centers closed until the end of the year. Because it will take at least that long until we have a vaccine. Italy has imposed a lockdown and has the opposite effect. They quickly reached their capacity limits, but did not slow down the virus spread within the lockdown.”
– Frank Ulrich Montgomery, German radiologist, former President of the German Medical Association and Deputy Chairman of the World Medical Association
“The range of predictions from virologists range widely. There are predictions that point to a disaster and there are predictions where the danger is relatively low and will end up being no more than a normal influenza season.” [adapted from the YouTube translation]
– Prof. Dr. Carsten Scheller, German virologist
“On the one hand, the media confronts us daily with alarming reports of an exponentially increasing number of ill and dead people worldwide. On the other hand, the media coverage in no way considers our required criteria for evidence-based risk communication.
[…] Data is provided without the necessary reference values. For example, it is said that ‘there are 10,000 cases so far’. Also, the naming of raw data without reference to other causes of death leads to an overestimation of the risk. In Germany about 2,500 people die every day. The data on deaths by Covid-19 should therefore be reported in the context of either the daily or weekly overall deaths in Germany. A reference to deaths from other acute respiratory infections would also be appropriate.”
“So I cannot answer my nagging doubts, there does not seem to be anything special about this particular epidemic of influenza-like illness.
Even though no one knows for certain how many people die of influenza every year, 2828 deaths in the space of three months compared to the nearly 900 000 deaths a month in China alone for all causes (mainly cancer and cardiovascular accidents) does not sound like much. And how do 86 deaths worldwide (excluding China) compare with deaths from influenza and influenza-like illness? Do not bother looking it up: we do not know.”
– Dr. Tom Jefferson, British epidemiologist, author and editor of the Cochrane Collaboration’s acute respiratory infections group, as well as part of four other Cochrane groups
“There is a lot of unjustified panic in Israel. I don’t believe the numbers here, everything is politics, not math. […]
To put things in proportion, the number of deaths of coronavirus in Italy is 10% of the number of deaths of influenza in the country between 2016-2017.
What we need is to control the panic. In the grand scheme, we’re going to be fine.”
– Dr. Michael Levitt, Professor of biochemistry at Stanford University and winner of the 2013 Nobel Prize in Chemistry
*Quotes taken from the Jerusalem Post and the Los Angeles Times
“[…] The Hubei outbreak – by far the largest, and a kind of worst-case scenario – appears to be winding down. How bad was it? Well, the number of deaths was comparable to an average influenza season. That’s not nothing, but it’s not catastrophic, either, and it isn’t likely to overwhelm a competent health-care system. Not even close.
[…] I am not preaching complacency. This disease is not going away any time soon; we should expect more cases and more local outbreaks. And COVID-19 still has the potential to become a major global health problem, with an overall burden comparable to that of influenza. We need to be vigilant in our surveillance.
[…] But we also need to be sensible. Quarantine belongs back in the Middle Ages. Save your masks for robbing banks. Stay calm and carry on. Let’s not make our attempted cures worse than the disease.”
– Dr. Richard Schabas, former Chief Medical Officer of Ontario, Medical Officer of Hastings and Prince Edward Public Health and Chief of Staff at York Central Hospital
“The debate and decision-making in the Corona crisis largely takes place without the participation of statisticians, epidemiologists, data protectors and data ethicists.
Distorted data, the quality of which is hardly suitable for decision-making, is analyzed in highly complex models as if it contained the urgently needed information we need to take action.
The negative consequences for social cohesion and prosperity are not well thought out. The political handling of the corona crisis in Germany has so far not been a lesson in responsible data use and data literacy.” [adapted from the Google translation]
– Frank Romeike & Katharina Schüller, experts in risk management and statistics
“[The research is] very biased. […] The chance of dying is […] standing at about 0.45 percent – very far from the World Health Organization’s [global mortality] figure of 3.4 percent.
[…] We won’t be able to isolate ourselves completely or forever. At some stage, we will have to resume a regular routine, and then the R0 will stabilize at 2 again. Effectively, we are delaying the inevitable.“
– Dr. Dan Yamin, PhD, infectious disease modeler and former faculty member, Center of Infectious Disease Modeling and Analysis, Yale University
“We no longer have to communicate the number of people who test positive to the new coronavirus. This is an improper use of scientific data which risks distorting not only the calculations on the size and lethality of the COVID-19 pandemic, but also give citizens the wrong impression, by conditioning their psyche and behavior.“
– Prof. Maria Rita Gismondo, virologist of the Sacco hospital in Milan
Additional sources for the quotes above: GlobalResearch.ca, Swiss Propaganda Research, and Off-Guardian.org
Touché. Me quoting all these contrarians is indeed showing my confirmation bias. I’m looking for evidence that my preferred outcome, “COVID-19 is not as dangerous as we think it is”, is true.
However, my goal in sharing these experts with you is to show you that unlike what is being displayed in the media, there are two sides of this debate. Not everyone agrees that COVID-19 is an extremely dangerous threat, and that the measures we’ve been taking to stop it so far are rational and based on sound scientific data.
| Bottom line: While the media has mostly ignored or even censored scientists and experts who express a view different from the current “corona-panic”, the calm, data-driven arguments they present won’t just go away, and need to be carefully looked at. After all, if the #1 worldwide expert in Communicable Diseases (Dr. Didier Raoult) says our reaction to this crisis is completely wrong… there might be something to it. |
Fact #7: The Data Confirms That Lockdowns Are Possibly Useless & Surely Damaging
Locking down an entire country to combat a virus was never considered the main strategy until the COVID-19 crisis, and yet somehow, now people tout it as the only logical solution there ever was, even going as far as claiming that’s something we’ll likely do forever.
We’ve already established the fact that we’ve successfully crashed the economy in a record time, and that we’ll have to deal with the consequences for a long, long time. But are those extreme measures really scientifically sound and necessary? And how will we assess how much such measures helped us save lives, or to the contrary, how devastating they were to the economy and the health of the entire population?
These are not easy questions to answer, and even less easy to ask — since the mere fact of second-guessing the current narrative on how effective the buzzword-strategy “Social Distancing” really is, can lead in this fear-driven climate to public shame, ad hominem attacks or even worse.
Using lockdowns to “Flatten The Curve” is a theory, not a scientifically-proven strategy
On March 13th, Dr. Neil Rau (infectious diseases specialist and medical microbiologist) and Dr. Susan Richardson (retired infectious diseases specialist and medical microbiologist who headed the Ontario Laboratory Working Group for the Rapid Diagnosis of Emerging Infections during the 2003 SARS outbreak) reminded everyone that:
Having failed to stop the virus completely, the WHO has revised the containment strategy to a novel one: to ‘flatten the outbreak curve’. This new strategy is being used to invoke severe restrictions to movement and liberty at an early phase of the pandemic in North America, although the effectiveness of this approach is unproven.” [emphasis mine]
In their opinion, “the WHO should abandon the containment ideal and urge countries to focus on how to best identify, prevent and treat the infection in the population that’s most at risk, in addition to protecting staff and patients in hospitals and the broader health-care community.”
They’re not alone, and the vast majority of the experts I’ve cited in the previous section (fact #6) claim that the current measures are “counterproductive”, “unreasonable”, “completely exaggerated” or even “suicidal”, and that in the end they “may not be worth the costs it imposes on the economy, community and individual mental and physical health”.
Of course, you can find other scientists who might think that the current measures are perfectly sound. But the fact remains that as Jefferson and his colleagues pointed out in 2011 — after doing a systematic review of “physical interventions to interrupt or reduce the spread of respiratory viruses” — the only 3 interventions that have been proven to reduce the transmission of viral respiratory disease are:
- frequent hand washing with or without adjunct antiseptics;
- barrier measures such as gloves, gowns and masks with filtration apparatus; and
- suspicion diagnosis with isolation of likely cases.
The effectiveness of other interventions are up to scientific debate, a debate that might unfortunately get you flagged as a “COV-idiot”.
A lot of questions remain unanswered:
- Are lockdowns or social distancing measures effective to reduce the transmission of viral respiratory disease?
- How long should lockdowns last?
- When and how will we know that a lockdown has been effective, and that it’s time to re-open the country?
- What will happen when we reopen the country?
- What will we do if there’s a second or even a yearly wave of COVID-19? Will we be locking down entire countries every single year?
- Is closing down schools even effective?
- Why have certain countries not imposed any lockdown and are still not seeing an increase in overall mortality from respiratory infections?
- What are the side effects of such interventions?
- How will we ensure that the application of unprecedented mass surveillance measures (China, South Korea, and many other examples come to mind) do not lead to further loss in privacy and individual rights, or of nefarious use of personal information by corporations or governments?
- Should corporations like Facebook, Reddit, Google, LinkedIn and Microsoft decide who can talk about COVID-19 and what can be said? Is this massive wave of censorship a philanthropic fight against misinformation or pure and simple corporate overreach?
The only way such questions will ever be answered is if we openly debate these topics, and certainly not by resorting to personal attacks, censorship and hatred.
The inconvenient truth: social distancing and lockdowns will kill people
I’ve heard a lot of people passionately use the argument “every life counts” when debating with someone who doesn’t agree that current lockdown measures are granted.
I am a humanist and value human life way more than money. However, most are forgetting that the side effects of lockdowns will themselves be deadly to some people — and that’s my biggest personal concern at the moment.
What are the consequences of an economic collapse, on the mental health of people, in a country like the US where suicide is the 10th leading cause of death, and considering that suicides are known to spike during these hard times?
If we apply the math found in the study above, and that the rise in suicides is equivalent to the Great Depression, we could expect the economic devastation related to COVID lockdowns to cause an additional 26,400 suicides per year.
But a financial crisis also affects every single citizen who goes through it for a long time, so much that it can reduce their life expectancy. Philip Thomas, Professor of Risk Management from the University of Bristol, warns that the 2008 Financial Crisis caused a 3 month decrease in overall life expectancy.
If we consider that every US citizen (329.45M as of August 2019) cuts 3 months off his life, and that the average lifespan in the US is 78.9 years, then the COVID-19 lockdown measures and its associated financial crisis might already have wasted 82,362,500 years of lifespan, the equivalent of 1,043,844 lives, in the US alone.
I realize this math might look just as speculative and sensationalistic as the one used in the media throughout the COVID-19 crisis, but it does prove a point: We absolutely need to consider the risk/benefit ratio of massive interventions such as the ones that have been taken in the last few months.
Political economist Toby Rogers, PhD, shares the same concerns:
There is a large volume of academic literature on “the social determinants of health” and “deaths of despair” caused by increases in the unemployment rate. The pioneering work in this field was conducted by Harvey Brenner (then at Johns Hopkins University) on behalf of the Joint Economic Committee of the United States Congress in the mid 1970s. Reviewing U.S. historical data over the period 1940 to 1973, Brenner found that:
‘… a 1% increase in the unemployment rate sustained over a period of six years has been associated (during the past three decades) with increases of 36,887 total deaths, including 20,240 cardiovascular deaths, 920 suicides, 648 homicides, 495 deaths from cirrhosis of the liver, 4,227 state mental hospital admissions, and 3,340 state prison admission.’
Based on the Brenner model, Rogers currently predicts that the economic crash following COVID-19-related lockdowns will in itself tragically kill a lot of people:
Lower bound. If the unemployment rate increases by 5 points as a result of the various lockdowns, then 294,170 additional lives will be lost, not from coronavirus, but from deaths of despair.
Mid-range. If the unemployment rate increases by 16.5 points (as predicted by Treasury Secretary Mnuchin), then 970,761 additional lives will be lost to deaths of despair.
Upper bound. And if the unemployment rate increases by 10-fold — which is what we are already seeing in several states — then 1,853,271 lives will be lost to deaths of despair from government orders to lock down, shut down, and shelter in place.
In a country where a record 3.3 million unemployment claims have been filed in the last week alone — up from the previous record of 695,000 in October of 1982 — saying the consequences of current lockdowns seem extremely dismal would be an understatement.

Several countries have been able to fight this crisis without destroying their economy
It would be silly to just argue that “we should have done what this country has done”. Every country is different, and the virus-fighting strategies that might have worked in one country won’t necessarily work in another.
That being said, the reality is that several countries didn’t have to impose extreme and damaging lockdown measures to successfully contain the spread of COVID-19 — which is not something often discussed in the media. These include:
If proper studies are funded, we’ll know what interventions were “worth it”, and which were not. At the moment, based on the data and facts presented in this article, my vague estimate is that lockdown measures are a mix of 20% social media trend, 60% political pressure and 20% science.
And since politicians, citizens and the vague majority of journalists reporting on COVID-19 have no idea that the threat is looking less and less dramatic the more data comes out, the interventions at the moment are exaggerated by default.
| Bottom line: Economy-crushing lockdowns and social distancing are the norm around the world, but have not been scientifically proven to work. Political pressure is at an all-time high, and at this point the actions taken to stop this so-called “deadly virus” are very likely completely exaggerated. |
Fact #8: Things Are Getting Better, And Better, And Better
On March 26th, the WHO’s Directed-General repeated that, “We are at war with a virus that threatens to tear us apart”, reminding everyone that “millions could die.”
These statements simply do not match the scientific data we have, which on the contrary is starting to support the idea that COVID-19 won’t likely be worse than a strong flu season. And considering that overall mortality from respiratory infections has still not increased significantly in virtually all countries faced with this “deadly virus”, the whole thing is starting to look like a big bubble of panic, politics and social media hysteria — a bubble filled with emptiness the menace of embarrassment.
The World Health Organization has reminded everyone that “facts, not fear will stop the spread of novel coronavirus” — and this entire article was my attempt to do just that.
New indications that the most dire movie-inspired scenarios based on the early, irresponsibly-shared, out of context case fatality rates shared by the WHO in early March will likely never become a reality are coming out every single day. But the media, citizens and politicians alike are repulsed and even angered by this inconvenient truth — since “it cannot possibly be true.”
And yet, the data (or lack thereof) is starting to speak extremely loud:
- As shared throughout this article, the real case fatality rates from COVID-19 will likely end up being very close to the seasonal flu once this whole thing is over
- It’s extremely unclear if what we claim are COVID-19 related deaths are in fact deaths from a slew of other factors, and if these deaths would have otherwise been “lost” in the midst of the 650,000 seasonal flu deaths or the millions of deaths from respiratory illnesses we see every single year
- The more we test, the more cases we find — a correlation which supports the idea that this pandemic is a pandemic of testing, and not the exponential spread of the virus
- More and more extremely credible experts are speaking out, even if they face the risk of losing their jobs
Dr. Ioannidis from Stanford went all out on March 26th, giving an in-depth interview where he admitted, yet again, that the data we are relying on to take decisions that will affect the entire society for decades to come is dramatically insufficient:
We need to act [based on] reliable data. Unfortunately much of the information that we have collected so far […] is not reliable. We have increasing evidence that many of the key features that pertain to what this pandemic is about, how lethal is that virus, how many people it has infected or will infect, what is likely to be the eventual impact and how effective are the different measures that we are applying… we have major gaps in practically all of those fronts. [emphasis mine]
I’ll end this section with a list of the latest “good news”, which I’ll try to keep updated as much as I can in the next weeks:
March 11th:
March 13th:
March 19th:
- “As of 19 March 2020, COVID-19 is no longer considered to be a high consequence infectious disease (HCID) in the UK. Now that more is known about COVID-19, the public health bodies in the UK have reviewed the most up to date information about COVID-19 against the UK HCID criteria. They have determined that several features have now changed; in particular, more information is available about mortality rates (low overall), and there is now greater clinical awareness and a specific and sensitive laboratory test, the availability of which continues to increase. The Advisory Committee on Dangerous Pathogens (ACDP) is also of the opinion that COVID-19 should no longer be classified as an HCID.”
- “Wuhan reported no new coronavirus cases today for the first time”
March 20th:
- “Japan was expecting a coronavirus explosion. Where is it?” Japan has basically done no testing at all, so it is not finding any cases. At the moment, no excessive mortality or clogged hospitals are being reported.
March 25th:
March 26th:
- “Imperial College scientist who predicted 500K coronavirus deaths in UK adjusts figure to 20K or fewer”. *That story was later corrected by researcher Neil Fergusson, who says that he expects the UK death toll to go down to 20k “in the presence of the very intensive social distancing and other public health interventions now in place.”
- A new study published by the University of Oxford shows that up to 50% of the population in the UK might already be immunized to COVID-19, and that only 1 out of every 1,000 people might need to be hospitalized. This contradicts predictions by the Imperial College, who predicted that up to 500,000 might die in the UK from COVID-19 if strong interventions are not being taken.
- Prof. Ioannidis from Stanford is featured in a long interview where he reiterates that the data we have is gravely insufficient, and that the interventions that are being taken might be doing more harm than good — we simply don’t know. He is the author of the controversial article “A fiasco in the making? As the coronavirus pandemic takes hold, we are making decisions without reliable data”.
March 27th:
March 28th:
- 2013 Chemistry Nobel Prize winner Dr. Michael Levitt argues that the COVID-19 pandemic will end soon.
- “The latest data from Norway, evaluated by a PhD in environmental toxicology, again show that the rate of test-positives does not increase – as would be expected in the case of an epidemic [emphasis mine] – but fluctuates in the normal range for coronaviruses between 2 and 10%. The average age of the test-positive deceased is 84 years, the causes of death are not publicly reported, and there is no excess mortality.” (Via SPG)
March 29th:
- Dr. Sucharit Bhakdi — one of the most cited research scientists in German history — published a video where he reiterates that “Implementation of the current draconian measures that so extremely restrict fundamental rights can only be justified if there is reason to fear that a truly, exceptionally dangerous virus is threatening us. Do any scientifically sound data exist to support his contention for COVID-19? […] The answer is simply: NO!” [emphasis mine]
- Dr. John Lee, retired professor of pathology and a former consultant pathologist for UK’s National Health Service, reiterates in an article that “Covid-19 deaths are a substantial over-estimate”, and that “the measured increase in numbers of deaths is not necessarily a cause for alarm, unless it demonstrates excess deaths [emphasis mine] – 340 deaths out of 46,000 shows we are not near this at present.”
- “The director of the University Medical Center Hamburg, Dr. Ansgar Lohse, demands a quick end to curfews and contact bans. He argues that more people should be infected with corona. Kitas and schools should be reopened as soon as possible so that children and their parents can become immune through infection with the corona virus. The continuation of the strict measures would lead to an economic crisis, which would also cost lives, [emphasis mine] said the physician.’ (Via SPG)
March 30th:
- Via SPG: “Professor Gérard Krause, head of the Department of Epidemiology at the German Helmholtz Centre for Infection Research, warns on German public television ZDF that the anti-corona measures ‘could lead to more deaths than the virus itself’.
- Yet again, “Covid19 yet to impact Europe’s overall mortality: Year-to-date statistics show excess mortality lower than previous years“
March 31st:
- I became aware of a March 19th editorial paper published by Stanford Professor John Ioannidis, titled “Coronavirus disease 2019: the harms of exaggerated information and non‐evidence‐based measures“. It’s a mandatory read to say the least, since Ioannidis explains in detail how the current corona-panic has led to a vast overestimation of how fast the virus spread, how deadly or dangerous it really is, and what evidence-based measures should really be taken to contain it.
- The COVID-19 situation is calming down in Italy, where the government is now starting to consider many options to end the nation-wide shutdown.
- Overall death rates are barely up in the UK for the past week, as reported by the Office for National Statistics. Once again, where are the extra deaths? Apart from a few isolated cases in France, Italy and possibly New York City, the COVID-19 global pandemic which was previously prophesied to kill millions and millions of people has still not been able to increase worldwide overall mortality rates.
April 1st:
- No, this is no April’s fool. Swiss Propaganda Research demonstrates that the list of Italian doctors who are claimed to have died from COVID-19 was quietly edited lately, and that their birth dates were removed. A lot of doctors on that list were 90+ years old when they died, and a lot of them did not even participate in the fight against COVID-19. (updated list here, original list with birth dates here. Thank God for Internet Archive…)
- A genetic analysis confirms that the severe cases of pneumonia reported in Italy before the COVID-19 pandemic (back in November and December of 2019) are officially due to other viruses. This supports the idea that severe pneumonia was already around in Italy before the COVID-19 pandemic and might have played an important role in the total death toll currently attributed to COVID-19.
- Social unrest is rising in Italy, and the side effects of the massive lockdowns that have been imposed are starting to be felt
| Bottom line: At the same time that emerging data is starting supports the idea that COVID-19 is unlikely to be more dangerous than a strong seasonal flu, most world leaders are running as fast as they can in the opposite direction. The best we can do is to wait until the data gets so overwhelming that the truth becomes self-evident: We can now stop panicking! |
The Anti-Conclusion: What This Article Does Not Claim
It’s not the first time I write something controversial, to say the least.
My 2017 book, The Non-Tinfoil Guide to EMFs (shameless plug, I know), talks about a topic — how wireless radiation and other types of electromagnetic fields impact our health — that most people consider akin to “ghost hunting”, but that is in fact extremely serious.
And I know by now that when you write something that goes against the grain, some appreciate you for it, and some hate you for it. Unfortunately, a lot of people who fall into the latter category try to put words in my mouth. An example,: “So, you’re saying that we should trash our phones and live in a cave?”.
To keep the discussion on this page constructive and open-minded, I’ve decided to include these “anti-conclusions”.
Here’s what the article above does NOT conclude.
- It does not argue that you should not respect currently mandated lockdowns or social distancing measures. This article is a call to openly debate what our next steps are, and an invite for citizens, politicians and everyone touched by COVID-19 (in other words… everyone) to review what the science actually says, and demand that our interventions become aligned with this new evidence.
- It does not argue that the virus SARS-CoV-2 does not exist, or that the associated disease it’s claimed to cause called COVID-19 does not exist. How dangerous this new virus really is remains up to debate, but it does seem to have unique characteristics different from other coronaviruses we’ve seen before.
- It does not argue that this is all a huge orchestrated conspiracy theory. There are surely financial interests at play here, but this speculation lies outside my area of interest and expertise. Future in-depth analyses might bring light to those highly important matters.
- It does not try to pin the blame on someone in particular, especially since we’re still in the midst of this crisis. After the fact, thorough investigation should be done to identify if special interests did play a role into either creating or perpetuating the panic we’ve experienced.
- It does not argue that people are not dying, or that it’s not tragic. Try to wrap your mind around the fact that every single year 2.6M people die from respiratory infections and up to 650,000 people die from the seasonal flu. That’s a lot of tragedy. Deaths from any cause are tragic, especially those that could have been prevented.
- It does not argue that doctors, nurses and medical staff are not fighting an incredible fight. Certain hospitals have become incredibly overwhelmed likely because of a combination of COVID-19 cases, general panic, and staff members needing to be quarantined for 2 weeks. My heart and gratitude goes to those who have been working exceptionally hard to save lives in circumstances that are extremely difficult.
- It does not argue that everything above is the ultimate “truth” and should be taken at face value. Things are evolving very fast, and facts presented above might change by the minute, so much that they might end up becoming half-truths. Don’t take my word for it and do your own research. Hopefully, what I’ve presented above and the experts with alternative point of views I’ve cited will help you in the process.
Conclusion: What This All Means & What You Should Do
This article demonstrates that COVID-19 probably represents a threat way less serious than what has been reported so far in the media, and that total lockdown measures might do more harm than good.
It’s unclear what measures should be taken — but it’s clear that we need to urgently demand that our governments listen to independent experts like Dr. Ioannidis from Stanford before taking further decisions.
An important action step I’ve seen many experts recommend to decision makers is to test a large random sample size of the population to be able to accurately assess: how many people are infected, how many have symptoms and how many die — in order to finally get a clearer picture of how much of a threat COVID-19 really represents. Iceland did an amazing job at this.
Prof. Sucharit Bhakdi proposes that we need to study a large group of COVID-19 patients to assess the real danger this new virus represents:
We need are 10,000 patients, all with respiratory tract diseases that are infected with common coronaviruses, and 10,000 infected with COVID-19. All with respiratory tract disease, nothing else. Then, we need to ask how many die in the first group, and how many in the second group. If the mortality is similar in both, then clearly they are similarly dangerous or less dangerous. Has there been such a study? No.
Note: the only study published at the moment which has compared the danger that SARS-CoV-2 represents compared to other coronaviruses is this French study I cited above, which concluded that COVID-19 has a death rate similar as other known coronaviruses.
It’s also clear that we need to have an open discussion about all this, because censorship or hatred will lead us nowhere. Incredibly profound questions need to be addressed:
- Is rushing the development of a COVID-19 vaccine so much that we skip key safety animal studies the only ethical thing to do, or a marketing move by those who will profit from it?
- Considering that we cannot keep the entire world on lockdown forever, what strategies might be preferable in the future if we see additional waves of COVID-19, or worse pandemics?
- How did the COVID-19 situation impact the fundamental rights that citizens should have in a free, democratic society? (you can read important discussions here)
- What are the true origins of the SARS-CoV-2 virus?
- How can we prevent a global panic during future pandemics? Who profited from the global panic, and who might have played a role in sparking it?
There are many, many rabbit holes you might want to go explore, depending on what you feel called towards.
If you liked it, please share this article with your friends and family members, but remember to respect their reaction — these are extremely difficult times for everyone and I know for a fact that the inconvenient facts I presented above will trigger a lot of people. The storm will pass.
Stay calm, stay home if that’s what is being mandated in your neck of the woods, and don’t forget to go outside (with the appropriate distance to other people if it’s mandated), get sunshine, walk barefoot on the grass to get your grounding on, meditate or partake in other activities you know can calm your mind, stay active, and do video calls with your friends and loved ones instead of staying alone. The storm will pass.
In the meantime, I’ll be here, at this computer, trying to make sense of the messed up and yet beautiful world we live in.
Yours truly,
Nick “The EMF Guy” Pineault
Special Thanks
Thanks M. for giving me a kick in the butt when I argued that I wanted nothing to do with this topic. Forty-five pages later, it looks like all I needed is to stop panicking and do what I do best — have a rational look at the data.
Huge thanks to Dr. Anthony G. Beck (AGB) and his Facebook group Balance Nation. I’m inspired by AGB’s courage to speak out and by his calm assessment of the situation, starting in early February.
Finally, I couldn’t have put together such a massive article without the help of the entire EMF Guy community, all the collaborators who helped me fact-check this article, David Crowe, Swiss Propaganda Research (SPG), Dr. Wolfgang Wodarg and investigative reporter Jon Rappoport.



67 Responses
Many thanks for this massive undertaking. I have read a lot over the last ten days and you have managed to condense much of it. Neil Ferguson did US no favours in the UK, predicting 250k deaths, which prompted our PM to go to lock down! There is so much evidence that 5G will have adverse affect on our immune systems – both in the UK and US, 5G continues to be ‘pushed’ out whilst most of the population are in lock down. Kind regards, Martin
Great point — the Imperial College model has been widely critized. I cannot myself do an in-depth critic of the model — I’ll leave that to scientists. But it’s a fact that scientists are not unanimous at all in supporting the decisions we’ve been taking and the interventions that have been done.
Overall, the article is excellent!!! ( a couple of minor typos, but nothing serious) I wish you had emphasized that a significant percentage of ‘affected people’ are ‘asymptomatic’,,, which sort of proves that by itself the problem is less than most folks are letting on,,,, and if we emphasized simple, proven preventative measures, (I think of Vitamin C, Zinc, and Selenium at minimum effective doses– All of which are cheap, readily available, and non toxic) a much greater percentage probably would be made asymptomatic. (That is, since most of the problem is connected to other contributing factors, helping the general health would probably weigh significantly in the balance,,, and be much less damaging than whatever ‘big pharma’ has or will come up with.)
Great point. I thought I had make that clear — I’ll add that in soon.
You sort of did say that,,,, but not so emphatically as I wanted to hear it… :-). Also, with an R naught of 4 (more or less, which was the first figure I read on it.) and a frequency of about 4 days, the entire world would now be inoculated, so the plague should be about over.
However, if the entire world were to be infected so quickly, emergency rooms would be overrun with those who did not have mild cases (and mild here can mean anything from no symptoms up to bronchitis and milder cases of pneumonia that don’t require oxygen or other breathing interventions). Deaths then would be in the range of some of the dire predictions.
Having any excess is always a danger. The way to avoid this is to support the system (with things like Zinc, Vitamin C,, Silver, Hydrogen peroxide, etc) to increase the percentage of cases that are minor or asymptomatic. In this particular case, since many are asymptomatic, and it is contagious without (or before) symptoms, it hardly makes sense to destroy the economy to work towards limiting contagion.
Thank you, Nick! I am sending this to my entire family.
Glad you liked it Julie!
Thanks for the in-depth look at massive statistical confusion! You make many salient points. The information is so important, but I think the fear tactics will prevent most from embracing true intellectual discernment.
Glad you liked it Kristine!
Thank you very much for the many excellent points in your article, however please also see explanation from Dr. Paul Cottrell why Covid-19 is MUCH worse than the flu…”Coronavirus Update: Dr Paul Cottrell: “Prepare NOW for 18 Months!” https://www.youtube.com/watch?v=J6VEYzwSdZU
Bonjour
Merci d’avoir investi tant d’énergie à la préparation de ce document. Cela donne espoir. Plus de gens seront au fait du contenu de votre compilation d’information, plus cette crise en sera abrégée.
Par vos noms, je déduis que vous êtes francophones. Qu’en penseriez-vous d’informer davantage de vos compatriotes de ce merveilleux contenu en ayant une version française de votre site web : n’est-ce pas là le but ultime de votre démarche ?
Je vous remercie de nouveau et laisse à vos bons soins de considérer cette démarche.
Bonne journée
I read this just to brush up on my french.
Oui je suis Québécois. Je n’écarte pas la possibilité de traduire certaines parties de mon site web en français, mais pour l’instant je n’ai pas les resources nécessaires pour le faire.
Super! Il y a beaucoup de potentiel, le français est une des langue les plus utilisée dans le monde. L’information que vous diffusez est vraiment importante et serait certes appréciée par tout ceux qui ne comprennent pas l’anglais. Bravo aussi pour votre site, j’aime bien le style épuré. Bonne fin de journée.
Great work Nick as always. Thank you so much for your valued time and your interpretation. Namaste, Tammy
Glad you liked it Tammy!
Amazing research Nick.
One other factor worth considering is how sleep influences survival chances with all infections.
From medcram: https://www.youtube.com/watch?v=G1zsE9_85i4
Since non-native EMF decreases sleep quality and efficiency it seems obvious to me that creating an EMF free sleeping environment is even more critical than ever.
Thanks for all of your research Nick. Some of what you pointed out with your research was an assumption of mine all along. At any rate I just hope and pray that this chaos will come to an abrupt stop and the truth will be uncovered and those responsible for falsifying and provoking panic will be brought to justice. Shameful we live in a world like this. BTW…. your new website is cool. It looks great. I wish you well.
Glad you appreciated it Tammy!
Thank you for putting this together,Nick . Finally, a rational compilation of balanced thought against all the fear and hyperbole out there!! I felt like the lone ‘crazy’lady’ out on my own trying to bring reason to those around me. Thank you for spending the time to put this all together. It is JUST what I needed. I, too, will be sending this out to family and friends. This article is like a deep breath of fresh pure air. :).
Thank you, please feel free to share it!
Great article!
Every time I switch on the TV, only to be told that the world as we know it has ground to a halt and the virus is on course to wipe out every person it touches, I can’t help wondering how the infected Boris Johnson is still running the country.
Thanks for the appreciation Bill!
The article is interesting, and not easy to decide wether coronavirus is a hoax or a pandemia. However before you believe the arguments listed in Fact #3 please read this fact based articel from Italy from the little town of Nembro.
“The real death toll for covid-19 is at least 4 times the official numbers.”
https://www.corriere.it/politica/20_marzo_26/the-real-death-toll-for-covid-19-is-at-least-4-times-the-official-numbers-b5af0edc-6eeb-11ea-925b-a0c3cdbe1130.shtml
Regards Gyorgy
Wow! What an undertaking! Congratulations on a well-researched and well-presented article that has been sorely missing in mainstream media. Definitely one to share widely whatever one’s perspective. Thank you.
Thank you very much Barbara! Feel free to share it to family and friends
Nice article, Nick! A great kick-off for your website. I’ll pass this along, even though I know it will “trigger” a few rascals I know. So far, the worst thing about this pandemic for me was that you had to go back to Canada too early! Oh well, I got in a nice hike that day anyway.
Appreciate it Pat! Feel free to share!
I really appreciate the research that went into compiling this article and will definitely spend some more time with it. However, I do think it would bring some balance to include descriptions from a few medical professionals who have witnessed in person the way that this virus operates when someone is dying from it. It is unlike anything they have seen before and it is eerily consistent from patient to patient once the disease progresses to the point of needing a ventilator. After hearing a CNP who has worked in ER and ICU for over 10 years describe it, I do not think that they are confusing the cause of death in these cases. I do acknowledge that what medical professionals are witnessing and what is being reported can be vastly different. As we look for more scientifically responsible reporting and solutions, we cannot disregard the science that is being observed on the front lines that is truly scary.
This is a great an important point, thanks for chiming in. There’s a lot of confusion and these clinical signs cannot be ignored. Since death certificates in Italy show that 88% of “COVID deaths” are in fact from something else, there’s also a lot of work that needs to be done to elucidate how many additional people are dying from COVID-19 compared to other known causes of respiratory failure (including seasonal flu, bacterial infections and many others).
Hello Nick, I appreciate your article. Thank you for all you put into that. My question though is with your premise that the response to Covid 19 has created economic ruin for the world. Has it? Is there evidence of the ruin? There is incredible funding channeled to various efforts, individuals, and businesses, which in the end go back into the economies of the world. Is this not correct? Am I being naive?
Thank you for this truly impressive article, Nick. Very well researched and thought out….It confirms with facts and data what my inner radar has been telling me all along…
Thanks for the appreciation Krista!
This is the best article I’ve read on this subject. Thank you!
Glad you liked it!
Thank you. I have been looking for this comparison data. The data in the media was useless to figure out what was really going on with the virus.
Glad you liked it Kris!
How is it possible that so many are treating the ‘numbers’ as accurate given the inaccuracies …. i.e. false positives and negatives …. you have indicated exist? With so much ‘uncertainty’ in the information there can not be any meaningful integrity to the published numbers or the results of the various simulations.
Well said. There is much speculation. What I see missing here is the flip side of the coin, those who may have COVID-19, but where never tested and therefore not counted (this could include some deaths). It will take another year before we have anything resembling conclusions without a large margin of error.
That’s a good point, although less likely because the more suspected cases are being tested. Also, if ‘they’re’ trying to inflate the death rate, they don’t want to test those in better health.
Correct, there is no meaningful integrity in the numbers. Many aren’t necessarily ‘treated’ either, many are asymptomatic, or just resting at home like you would with a flu. I did all this work looking into the PCR test and the inventor Kary Mullis said it’s not meant for this application (among some other interesting points…), but really the kit says it’s ‘not meant as a diagnostic tool’. So why is this being used? because it can show almost any infection (ex. common cold, other corona viruses) or other factors as a positive. A good joke I saw was “basically anyone with an immune system” can test +ve :D
Nick, IMO, you did a brilliant job at putting such a comprehensive piece together! The thoughtful manner in which you have assembled and structured the massive amount of information on this perplexing subject, permits one to have a step back from the extremely complex situation at hand, to get more of a wide angle view. I, for one, very much appreciate that you’re a self-professed contrarian. The “official” narrative is so ubiquitous, pervasive and aggressive via the MSM outlets, that it just might be analogous to getting waterboarded, where the water is one relentless narrative being pushed, not down your throat, but into your psyche. This behaviour does give one reason to wonder what’s the actual intention underlying what sure seems to be a grossly disproportional reaction to the situation.
As a side note: speaking of “official” narrative…any society where the official narrative is being elevated to be “king of the mountain,” and the society is actively suppressing (overtly or covertly) any narrative that is contrary to its own, is a society on the way down and out. Such a society is so off-balance that it is impossible to sustain. A society in this condition is the spinning top that has moved away from an equilibrium of forces, begins to wobble and eventually topples over.
Your article, Nick, appeals to the free-thinking individual and the free thinking individual will get it and understand its value. All those links…so many rabbit holes to explore! I also see your article, as it is not being driven by misemotions, nor is it abrasive in its presentation, to be an article that will be appropriate to disseminate to a wide audience that represent diverse perspectives, that are wanting to know and understand what’s really going on with this pandemic.
Japan just annouched a state of emergency today they currently have 4,600, with 91 deaths. Don’t worry you still have Singapore and Taiwan, for now
It’s not because you have 91 people die (keeping in mind that a lot of these confirmed deaths might not be COVID related at all — but let’s say we put that argument aside) that you’re “proving” that COVID-19 is as dangerous as everyone makes it to be. In a large population like Japan (126+ millions), a few thousand deaths from COVID-19 wouldn’t be surprising.
Even then, if the overall mortality rates don’t increase, these so-called COVID-19 related deaths would have otherwise be flagged as something else if we weren’t so myopically focused on covid right now.
People freak out over the number of “cases”, but a case doesn’t mean “symptomatic”, “hospitalization” or “death”. If you test, you find cases.
“Based on reports from the designated facilities, it is estimated that 2.23 million people underwent medical consultations in Japan for influenza from January 21 to 27, an increase compared to the 2.13 million estimated for the previous week.” https://www.nippon.com/en/japan-data/h00386/japan-gripped-by-major-flu-outbreak.html
We need to put things into perspective. Don’t let yourself be caught in the fear mongering and be distracted by big words like “state of emergency”.
this is the most ridiculous and dangerous misinformation i’ve read yet.
Anyone can say that anything is “misinformation”. Please explain your point: what part of what is presented do you not agree with?
Awesome overview Nick, thank you so much for your hard work on this!! So here’s a question I need help understanding: assuming that the virus is not nearly as serious as projected, how do you explain what’s going on in New York? Many deaths, overwhelmed hospitals, and many young people dying…thoughts?
Hey Cathy,
This is speculation — since I don’t have the “ultimate truth”, but what I think is happening is:
– Some hospitals are overwhelmed, and some are not. The media are clearly highlighting those who are overwhelmed since it helps fuel their crazy scary narrative.
– The panic is contributing to the overwhelmed hospitals. This is true all over the world in ICUs that are already nearing full capacity every Winter. NYC hospitals seem to have run at 80%+ capacity in 2018 https://council.nyc.gov/budget/wp-content/uploads/sites/54/2019/02/Health-and-Hospitals-Hospital-Utilization-Report.pdf (I don’t have time for a thorough research on this, I’d need to find several sources to be more accurate.) It’s a known fact that Italian ICUs run at 95-98% capacity every Winter. Add a little bit of panic or extra illness and they are overwhelmed. Italians ICUs have been known to refuse some people in harsh flu seasons — so this sort of overwhelm can and does happen outside of any COVID situation.
– Staff members that are tested positive need to be quarantined. Another contributor to
– A lot of what is currently flagged as covid could be something else. In Italy, only 12% of all COVID-related death were found to be causative. This number might change after there are further investigations, though.
At the moment, pneumonia-related deaths have not increased in the US. There’s delay in reporting so at the moment we cannot say whether COVID-19 has led to an increase in overall mortality or mortality from respiratory illnesses in the US.
If, like most of Europe and like most other countries, COVID-19 doesn’t contribute to a VAST increase in overall mortality (“excess mortality”), then our current interventions and their related consequences on health and wealth are likely doing more harm than good.
Ok, good insight here. Thanks again for your thorough investigation on this. I truly hope we start to see some more honest conversations and that this message gets out there.
This is a great article and I have shared it on Facebook. I am a Functional medicine practitioner
and would like to offer a free consultation to anyone wanting to learn more about how to have Vibrant Health without disease at any age. My email is [email protected]
Your source interview with Dr. Schabas from Toronto was quite old in terms of the epidemic. It also contained the following quote: “Could the situation change? Could COVID-19 become a true pandemic with millions of cases and tens of thousands of deaths every day? Of course. The current situation in Italy particularly is concerning. But as the days pass and the global patterns stay the same, this becomes less and less likely”. Unfortunately, the situation did change and the pattern of 10,000 new cases a day world wide increased dramatically. As much as I want to believe your narrative, and as much as my initial thoughts a month ago aligned with what you have posted here, the current situation is concerning.
Hi Nick,
My nature is not contrarian but instead I seek out balance and truth from the perspective of truth being found in the center of ‘what is’ as opposed to the perimeter. And so I find your article both irritating and important at the same time. Important because too many people ‘seem’ to be on one side of the boat and you’re on the other side waving for support before thing thing tips or is damaged beyond repair (or a multi-trillion dollar price tag). Irritated because your position is still not coherent. You’re like a trickster dancing in the streets telling the people they’re all crazy but when they look to you your message is just smoke and mirrors. There’s no answer but an emotional wrench to challenge the conventional wisdom, not to contribute in a meaningful way. Unless you consider the roll of the trickster meaningful. Which I do. Hence important and irritating. Aho!
Mark
A very well written article,thankyou, but… you’re the EMF guy and you didn’t see a link between radiation/microwave sickness and the symptoms of Coronavirus? Not even a mention? You’re the EMF guy…
https://blog.nomorefakenews.com/2020/04/07/covid-and-a-5g-connection/
https://youtu.be/1EWQPgF6-UQ
http://www.radiationdangers.com/5g/is-the-coronavirus-actually-microwave-illness/
https://www.princess.com/ships-and-experience/ocean-medallion/medallionnet/
Lockdowns have been used extensively in the past, for example, with the Spanish Flu. It’s not an untested method, and it had positive results. People also knew to wear masks back then, but the WHO and CDC missed that memo.
Sweden looks significantly worse than its neighbors: Denmark, Finland, and Norway. Certain countries, such as the UK, Spain, and Italy, already struggled to handle the influx of patients. Assuming no lockdowns would have doubled or tripled their mortalities (which is actually being generous because Sweden is well beyond those numbers compared to their neighbors), it would have been a disaster.
I think we could have learned from Taiwan, but they were mass producing masks from the start, rationing them to the citizens, taking temperatures before entering buildings, etc. The lack of organization in many Western countries is a disgrace. S. Korea’s model probably can’t be copied, an incredibly high level of tracing. Iceland has an extremely low population density which probably lowered the rate of spread (compare to NYC), and their testing per capita is second to none. The model that a country like the U.S. should follow doesn’t really exist, which is part of the problem.
Also, for the CDC numbers, you’re comparing confirmed influenza cases with estimated influenza deaths. There’s only around 5k confirmed influenza deaths per year in the USA, the 23k was the CDC’s estimate. Anyway, a lot of other numbers have changed since your post as well. The UK, for example, declaring the disease was no longer a great concern is somewhat ironic since they just had their two highest all-cause mortality weeks this century.
The smog, I think it’s a valid co-factor in worsening COVID-19 symptoms, but did it just suddenly appear in Italy these past few months? We can track their all-cause mortality in previous years, influenza should be worsened by smog as well, yet we’re not seeing the same numbers during peak flu season. Smog could be a contributing factor, but to suggest it’s the major factor seems off-base.